


The inventor of auriculotherapy, the Frenchman Paul Nogier (1908-1996), was born in Lyon where he studied engineering and later read medicine. His concepts are based mainly on two assumptions: that the human outer ear is an area where the entire body and its internal organs are projected, and that, by stimulating specific points on the outer ear, therapists influence the health and function of inner organs and other body parts that correspond to these points.
The history of Nogier’s auriculotherapy is intriguing. As a young doctor, Nogier observed that some of his patients had a scar on their ear. He was told that an alternative therapist, Madame Barrin from Marseille, had been cauterising a certain spot on the ear (later called the Barrin point) in the belief that this would alleviate the sciatica symptoms of these patients. Nogier was fascinated; after inserting needles in this spot, his sciatica patients seemed to experience improvements of their back pain. If one specific area of the ear could be stimulated to alleviate sciatica symptoms, Nogier wondered, would different areas of the ear be useful for treating other parts of the body?
Nogier soon believed to notice that the “Barrin point cauterisation technique” only worked for sciatica and not for hip, knee, or shoulder pain. He thus concluded that the Barrin point on the ear corresponded to the lumbosacral area where the sciatic nerve leaves the spinal canal. The protruding part of the ear – the antihelix – might then correspond to the spinal column, Nogier speculated.
He soon thought to discover that the outer ear had exceptional reflex properties, and that each point in the ear pavilion was related to a specific part of the body. Eventually, he came to the conviction that the entire human body was sketched out on the ear with the lobule at the bottom of the ear corresponding to the head; the concha in the centre corresponding to the thorax and abdomen; and the cartilaginous portion, the antihelix, corresponding to the spinal column.
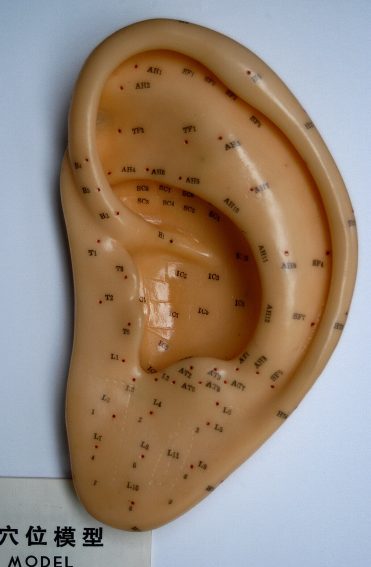
To identify the most crucial points, Nogier used an electronic device that allegedly measured cutaneous conductivity. In this way, he managed to develop a detailed ear chart. Nogier became convinced that the ear is energetically related to other parts and organs of the body, corresponding to an upside-down foetus. He also came to believe that, when applied to the outer ear, specific frequencies cause specific effects on the body, and that by stimulating the correct point of the ear, one can treat problems of the corresponding body part. He was further convinced that, through auricular diagnosis, he could identify a range of chronic illnesses.
Even though far-fetched and bizarre, Nogier’s concepts were widely accepted in the realm of so-called alternative medicine. Yet, they were ridiculed by scientists because they were not in line with the existing knowledge of anatomy and physiology. Moreover, the different maps used by proponents of auriculotherapy showed embarrassing disagreements. In other words, the assumptions of auriculotherapy lacked both consistency and plausibility.
But CAM proponents rarely allow the truth to interfere with their beliefs. Today, auriculotherapy is being promoted as a panacea, a treatment for most conditions. One of the first rigorous tests of auriculotherapy was published in 1984 by one of the most prominent researchers of pain, R. Melzack. He concluded that “auriculotherapy is not an effective therapeutic procedure for chronic pain”.
Since then, an abundance of clinical trials has emerged. Their results are confusing and by no means uniform. It is therefore wise not to rely on single studies, but on systematic reviews that include the evidence from all reliable trials. One such review concluded that:
because of the paucity and of the poor quality of the data, the evidence for the effectiveness of auricular therapy for the symptomatic treatment of insomnia is limited.
An in-depth assessment of the evidence entitled “Évaluation de l’efficacité de la pratique de l’auriculothérapie” was carried out in 2013 by Inserm at the request of the French Ministry of Health. It failed to demonstrate the superior therapeutic effect of auriculotherapy compared with placebo for most of the claimed indications. Other authors arrive at more positive conclusions; however, due to the often poor quality of the primary studies, they should be interpreted with great caution.
Contrary to what auriculotherapists try to make us believe, auriculotherapy is not free of risks. The most frequently reported adverse events include local skin irritation and discomfort, mild tenderness or pain, and dizziness. Most of these events are transient, mild, and tolerable. Sadly, this does not mean that auriculotherapists do no harm. Whenever they advocate auticulotherapy as an alternative to an effective treatment for a serious health problem, they endanger the health, perhaps even the life, of their patients.
So, the final conclusion can hardly be positive. The effectiveness of auriculotherapy has not been demonstrated beyond reasonable doubt. The treatment is associated with considerable risks. Therefore, its risk/benefit balance fails to be positive.